J. Borgstein & C. Grootendorst, The Lancet 2002; 359: p473
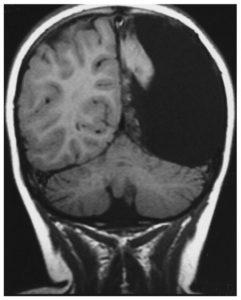
Infants and young children do surprisingly well after the surgical removal or disconnection of up to half of their brain. Most can talk, walk and even run. These exceptional children are proof of baby brain neuroplasticity. This heroic surgery is done to treat severe, uncontrolled seizures. If the seizure focus is confined to one side of the brain, taking out the damaged part works well. Studies have shown that most of the children can talk and if they have good therapy post surgery, their walk can be virtually normal. 1
How do they do it?
After the hemispherectomy, the remaining half a brain grows and rewires so that one side of the brain can control both sides of the body. This works very well for the legs, but for most children, leg function is overall better than arm and hand function on the affected side. Just as in a child with hemiplegia, after a Grade IV hemorrhage or severe PVL, the leg is usually more functional than the hand. Ninety nine percent of children with hemiplegia will ultimately walk 2 and most will run better than they walk. 3 (Baby Brain Neuroplasticity)
Why the difference?
Part of the answer is explained by differences in the wiring patterns in the brain between the arm and the leg, but part of it is activity dependent neuroplasticity. You need two legs to walk but one hand is good enough for most functions. If an adult loses a leg in an accident, it is worth a lot more money in compensation than losing an arm.
In my book, I devoted an entire chapter to explain the concept of developmental non-use, which happens when the child preferentially uses the hand that works better and neglects the more affected one. (The Boy Who Could Run, But Not Walk) Developmental non-use is a simple example of the use it or lose it phenomena in brain development.
What if we force the use of the neglected hand?
There are multiple Randomized Controlled Trials of Constraint Induced Movement Therapy (CIMT) that have demonstrated that a short 2 to 4 week intensive training period can improve hand function and that this improvement is maintained after the intensive. The most exciting data is that this very short period of intensive training also rewires the brain.4 These studies prove that early neglect can be overcome by activity-dependent neural plasticity. It takes time and work to overcome an early-learned habit, but it can be done.
More on this next week.
- Mark W. Burke, Ron Kupers, and Maurice Ptito, “Adaptive Neuroplastic Responses in Early and Late Hemispherectomized Monkeys,” Neural Plasticity, 2012 (2012), Article ID 852423, 12 pages.
http://www.hindawi.com/journals/np/2012/852423/cta/
- Iona Novak, “Evidence-based diagnosis, health care, and rehabilitation for children with cerebral palsy”, Journal of Child Neurology. 29 (2014): 1141-1156.http://jcn.sagepub.com/content/29/8/1141.short#cited-by
- Frank S. Pidcock et al, “Pediatric constraint-induced movement therapy: a promising intervention for childhood hemiparesis”, Topics in Stroke Rehabilitation. 16 (2009): 339-345.http://www.tandfonline.com/doi/abs/10.1310/tsr1605-339#.V4Um8Ffyop0
Fascinating. I have seen a first hand account of the power of these methods of re-wiring a young brain, It is miraculous. Thanks for the explanation and giving hope to others whose children may seem to be facing insurmountable problems. It really is a case of “where there is a will, there is a way!”
Hello Bernie, Thank you for your email.I am sure as we look about us, other cases of remarkable recovery will emerge. These Outliers have another important role to play; they teach us what the brain is capable of accomplishing. Our collective goal must be to figure out the best ways of stimulating recovery in other children.