Doing “more of the same harder” is unlikely to produce significant change. Why not try something new this summer? Traditionally, most doctors and therapists have focused their work on the area of most involvement. For children with cerebral palsy at Level I to IV, I am suggesting that you turn this upside down and work on the least involved parts of the body.
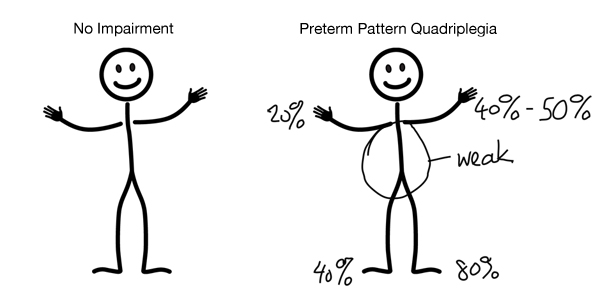
The first step is to look at the whole child and assess the degree of impairment in function in each area of the body. I have used a scale of 0 to 100% for full impairment. The stick figure represents a child with cerebral palsy. The diagnosis is preterm pattern quadriplegia with more impairment in the legs than in the arms.
Cerebral Palsy: The Timing of Damage is Important
The pattern is asymmetric, with more impairment on the left than on the right side. This 6-year-old child is able to walk, in a walker, for short distances with difficulty.
At 20%, the right hand has the least involvement. She can use it well when sitting, but it tightens up enough to make her grasp clumsy when she is upright. It is functional to hold and steer her walker. The left hand (40-50%) is a useful helper hand when sitting, but needs a Velcro band to hold it in place when she uses the walker. There is a clear “activity dependent” increase in tone in both hands when she is up and walking.
She has bilateral hinged AFO’s even though there is a marked difference in the degree of impairment between the 2 legs. The trunk is weak, which is so common as to be an almost universal finding in children with 4-limb involvement.
This child has had twice a week PT and once weekly OT from 3y onwards. In Grade 1 she had difficulty keeping up, requiring help and supervision for movement. The school is requesting wheelchair use when she goes back to school after the summer.
What can be done to make her more independent over the next 2-3 months?
Her body alignment is in good shape, thanks to a regular massage and stretching program as well as a few rounds of Botox to her leg muscles.
I would start by stabilizing her trunk with a compression garment. I would expect the posture to improve and the “activity dependent” tone in her hands to decrease if the support is supportive enough.
Good Enough Is Not Good Enough Any More – Function Follows Form In Cerebral Palsy
Quick Fixes – Take Your Therapist’s Hands Home with You.
Here is the revolutionary idea. I would work with her therapist to give as much support as possible to her left leg. In addition to a stable AFO, I have used whatever degree of knee support that is needed to basically turn that leg into a stable “peg leg”. With one stable leg, I would focus on improving the strength and function of the less impaired right leg. At 40% of full function, there is less improvement needed to get into a normal range. Why do this? The answer is simple. All (98-99%) children with hemiplegia walk independently, only 23% of children with Quadriplegia manage this skill.
Will My Child Walk? Are We Doing the Right Therapy?
By focusing on the less involved right side, the goal is to change her from a quadriplegia to a hemiplegia pattern. Once she is able to walk on her own, the right side will naturally strengthen and function better. With more trunk and leg support, the tone in the arms and hands will decrease. Then the goal will shift back to improving the left leg.
Try rating your child or favorite patient this way and see what you find. For a child with asymmetric diplegia, this method works the same way. If the child is completely symmetrical, then I would chose to increase the support to the left leg and work intensively on the right as roughly 80% of us are destined to be right handed.
In full-term pattern quadriplegia or hemiplegia, the game plan is similar. Increase trunk support and splinting to the most affected limbs and try to strengthen and increase function in the less involved areas. Doing “more of the same harder” over the summer months is unlikely to make a big change! Print this blog and discuss it with your therapist. Your therapist can try out the effect of increased support with taping and air splints to see if it is worth the effort.
Send me your comments and questions. Remember, there is a growing amount of research that demonstrates children with cerebral palsy can show significant improvement in as little as 3-6 weeks with therapy that is novel, challenging and has observable benefit for the child.
Neuroplasticity and Hands: Doing The Right Thing, At The Right Time, and In The Right Order
With the right type of support in alignment, you can see significant change in days. Make this summer one of positive change.
http://www.sbstherapycenter.com/#!services2/cctp
Thank you again for posting your therapy specific ideas. There is so little practical dialog about what therapists actually do – as if physical therapy was a one size fits all prescription.
I usually agree wholeheartedly with your recommendations but this last post of yours left me unsettled. Too long to write in a comment so I thought I’d post a response on my blog.
http://wiredondevelopment.blogspot.co.nz/2015/06/constraint-induced-therapy-and-good-limb.html
Would love to know what you think.
Thank you for another insightful explanation of the ideas I am trying to put forward. My readers should also read you blog post at the link above. My first exposure to therapy in babies and young children was with Sarah Blacha Forsythe. When we first started to work together, Sarah had just taken one of the first Baby courses from Mrs Bobath. Together we saw the evolution of spasticity over the first years of life in a large number of “at risk” babies in the HSC Neonatal Follow-Up Program. So you are right. Using increased support on the most affected limb is a form of TIP (tone inhibiting posture) from classic NDT… Although I am old enough to still call it RIP(reflex inhibiting posture).Basically, splinting the most involved side breaks up the “Habitual” movement pattern and gives the child a challenge to move in a more appropriate way. Brains respond to novelty with increased neuroplasticity! Thanks again for your insight.